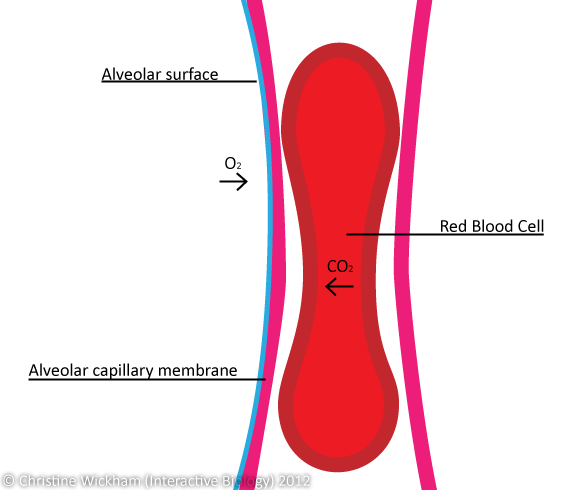
Gas exchange in the lungs occurs where there is both ventilation and perfusion (blood flow). Areas of the lungs in which gas exchange cannot occur are called anatomical dead space. This is because anatomically, gas exchange cannot occur anywhere other than the alveoli.
Gas molecules dissolve into the water that covers the alveoli and diffuses along a concentration gradient across the respiratory membrane and capillary wall into the blood. This is due to the partial pressure of oxygen in atmospheric air.
You may have encountered the concept of partial pressures in chemistry. Basically, in a mix of gases, each pure gas represents a part of the total pressure. Let us consider air — a mixture of oxygen (21%), carbon dioxide (0.03%), and nitrogen (78%) as well as a few other trace gases.
The atmospheric pressure of air is 760mmHg, since 21% of air is oxygen, 21% of 760mmHg is 159mmHg and thus, the partial pressure of oxygen in air is 159mmHg.
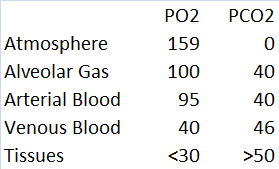
If you look at the table (image courtesy of the author for use on the Interactive Biology website) above, the partial pressure of air (PO2) of alveolar gas is 100mmHg as inspired air mixes with staler expired air. You may have noticed that the arterial blood has a PO2 of 95mmHg. This is because the respiratory system involves two blood supplies; the pulmonary circulation and bronchial arteries. The pulmonary circulation carries blood from the heart, through the lungs to be oxygenated and then back to the heart to be pumped around the rest of the body.
The bronchial arteries are branches of the thoracic aorta and they supply the lung tissues with oxygenated blood however, there are no veins to return de-oxygenated blood to the heart, instead the deoxygenated blood simply mixes with the pulmonary system, hence why systemic arterial blood has slightly less oxygen.
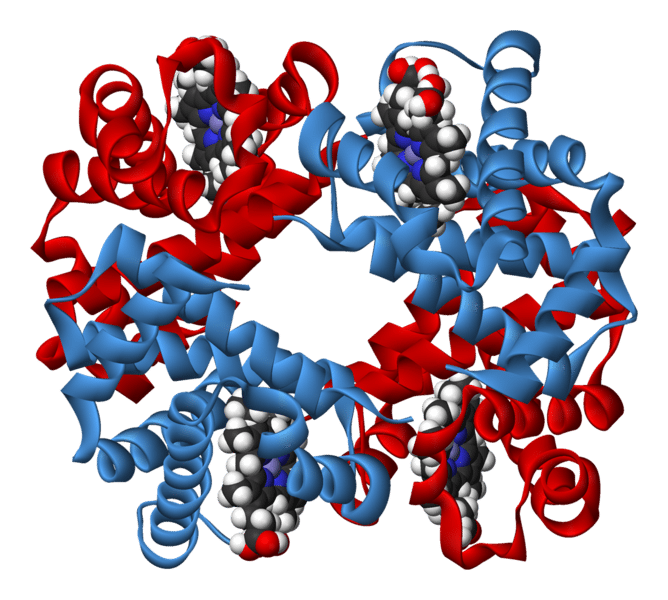
So what happens to oxygen when it passes through the alveolar membrane? Some of it dissolves into the water in the plasma; however, most of it enters red blood cells to bind with haemoglobin, each of which have four binding sites.
A vital concept in respiratory physiology is the oxygen-haemoglobin dissociation curve.
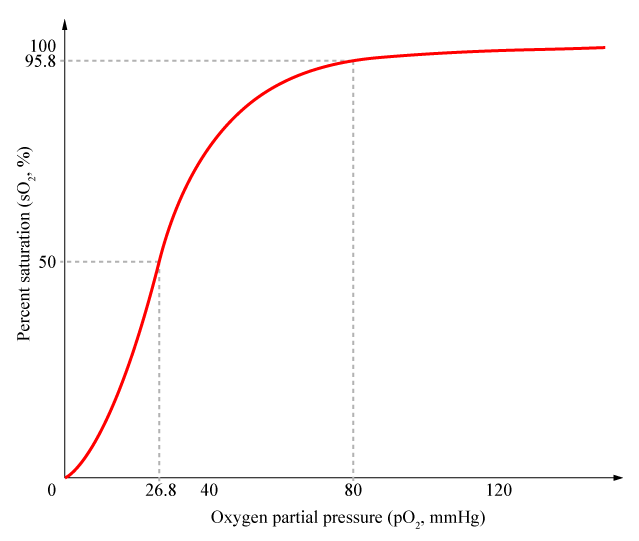
The shape of the curve shows us that the PO2 needed to load the first oxygen molecule onto haemoglobin is higher than that needed for the second to fourth molecules. This is because the binding of the first molecule alters the shape of the haemoglobin and facilitates the loading of the other three molecules. Once 95% of haemoglobin has been filled, it starts to get harder for oxygen to find empty binding sites to load.
The blood oxygen saturation of a regular, healthy person is 98% or higher. Saturations of <95% are considered abnormal and should be treated as with even a small decrease in PO2 can cause a rapid drop in blood oxygen saturation.
In my next article I will be talking about the factors that change this curve as well as CO2 exchange at the tissues.