Before we talk about “Marfan syndrome”, let’s look at the normal histology of elastic tissue, the tissue affected in Marfan Syndrome.
Elastic fibers are widely distributed all over the human body specially in skin, tendons, cartilage, muscle, blood vessels, dura mater, and suspensory ligament of lens. The integral components of elastic tissue are called microfibrils. The major building block of microfibrils is called fibrillin which is a glycoprotein encoded by FBN1 and FBN2 genes.
Fibrilin contains a type of monomer called Ca2+binding Epidermal Growth Factor (EGF). Calcium binding to these monomers stabilizes the microfibrils, and subsequently stabilizes the whole elastic tissue while calcium loss or mutation of fibrilin causes the microfibrils to disintegrate leading to weakening of the elastic tissue.
What is Marfan Syndrome?
- It is the most common connective tissue degenerative disorder. It is an autosomal dominant inherited disease.
- As you know, we have 23 pairs of chromosomes, 22 of them are autosomal while the remaining pair is concerned with identification of your gender, XY or XX. Marfan syndrome has no relation with these sex chromosomes. It only occurs due to mutation in an autosomal chromosome #15.
- Marfan syndrome is named after Antoine Marfan, the French pediatrician who first described the condition in 1896.

Abraham Lincoln
- Did you know that Abraham Lincoln (1809–1865), the 16th US President, is thought to have Marfan syndrome? Also, Nicolo Paganini, an Italian violinist and composer had Marfan’s.
Causes
Marfan syndrome results from mutations in the FBN1 gene (usually in the calcium-binding EGF portion) causing the microfibrils to lose their mechanical strength leading to:
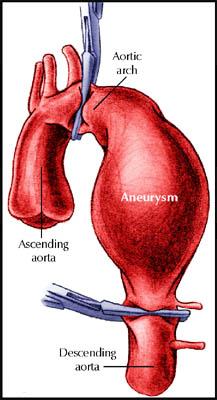
- Weakening of the aortic wall. Progressive aortic dilatation and aortic dissection occur because of tension caused by left ventricular ejection impulses.
- Reduced structural integrity of the lens zonules, ligaments, lung airways and spinal dura.
Genetics
- If one parent is affected, there is a 1 in 2 (a 50:50) chance that a child will be affected.
- Marfan syndrome is a variable disease. So, a child may be affected less severely, or more severely, than his/her parent.
- If a woman with Marfan syndrome becomes pregnant, the pregnancy can put an increased demand on the heart that may increase the risk of aortic rupture.
- The mutant fibrillin-1 disrupts microfibril formation through the other fibrillin gene encodes normal fibrillin, that’s called dominant-negative mechanism.
Clinical Findings
If you are a doctor and a patient with Marfan comes to you, you can diagnose him/her depending upon many criteria in skeletal, ocular, cardiovascular system or any other system containing elastic tissues.
At first, we’ll discuss the skeletal findings of such patient. The patient is usually taller and thinner than his/her family members. The following are some of the major criteria:
- Severe pectus excavatum or pectus carinatum(pigeon chest) in which the sternum is concave forward or convex forward respectively.
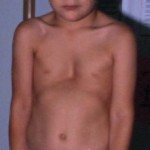
Severe pectus excavatum 
Pectus Carinatum (Pigeon Chest) - Arachnodactyly: the fingers are longer and will look like a spider’s fingers (Arachno – “spider,” dactyly – “finger”).

Arachnodactyly - Dolichostenomelia: limbs may be unusually long in proportion to the torso.
- Scoliosis (Cobb angle >20°)
- Reduced extension of the elbows (< 170°)
The following skeletal criteria are minor in Marfan: Joint hypermobility, highly arched palate, enophthalmos and retrognathia.
Secondly, let’s talk about the most serious findings of Marfan Syndrome which are usually the cause of death in these patients:
Cardiovascular findings:
 Major criteria:
Major criteria:
- Aortic root dilatation.
- Aortic dissections involving the ascending aorta.
- Minor criteria:
- Mitral valve prolapse.
- Dilatation of proximal main pulmonary artery.
- Dilatation of descending aorta.
Ocular findings:
- The major criterion is dislocation of the lens caused by weakening of the suspensory ligament. Dislocation usually occurs in the superotemporal direction.
- Minor criteria include: myopia due to increased axial length of the globe. Flat cornea also may be present.
Dural findings (Dural Ectasia)
- Dural ectasia is a ballooning of the dural sac and the spinal canal, often associated with the nerve root sleeves out of the associated foramina. It usually occurs in the lumbosacral spine.
- The most common clinical symptoms are low back pain, headache, rectal pain and pain in the genital area. The symptoms are aggravated mainly in the supine position and are relieved by lying on the back.
Treatment
- Back brace can help if scoliosis causes severe skeletal problems or pain.
- Surgery for pectus excavatum or carinatum, to prevent skeletal complications and to relieve pain.
- Annual eye exams become a must, as well as visits in between annual visits if any problems with eyesight are detected or suspected.
Hi Ahmed,
Thought I might mention that another significant issue that individuals with Marfan’s face is an increased risk of spontaneous pneumothorax.
Also that Marfan’s is an extremely rare condition that most hospital doctors will see only a few times in their entire careers if at all.
Great article though, it will definitely come in handy if I ever do a case-study on it 😛
Hi Christine,
I’m glad you liked my article.
of course there are many other symptoms that I didn’t mention here for the sake of simplicity like spontaneous pneumothorax, striae atrophicae. they are minor criteria occurring in small percentage of Marfan patients.
Feel free to use the article whenever you need it, its yours 🙂
Regards,
Ahmed
I was diagnosed with Marfan syndrome when I was nine. My father died from an aneurysm of the aorta. My question is if it is possible for hydrocephalus to have any connection with Marfan Syndrome? I am also having severe headaches.
Thank you
Holly 28
good presentation.plz update about the pathology details